Ebola protocol failure refers to the systemic collapse of containment measures when technical diagnostics are prioritized over basic health infrastructure. In the 2026 Bundibugyo outbreak, this failure was evidenced by the virus circulating undetected for weeks despite high-resolution surveillance systems, ultimately breaching international borders.
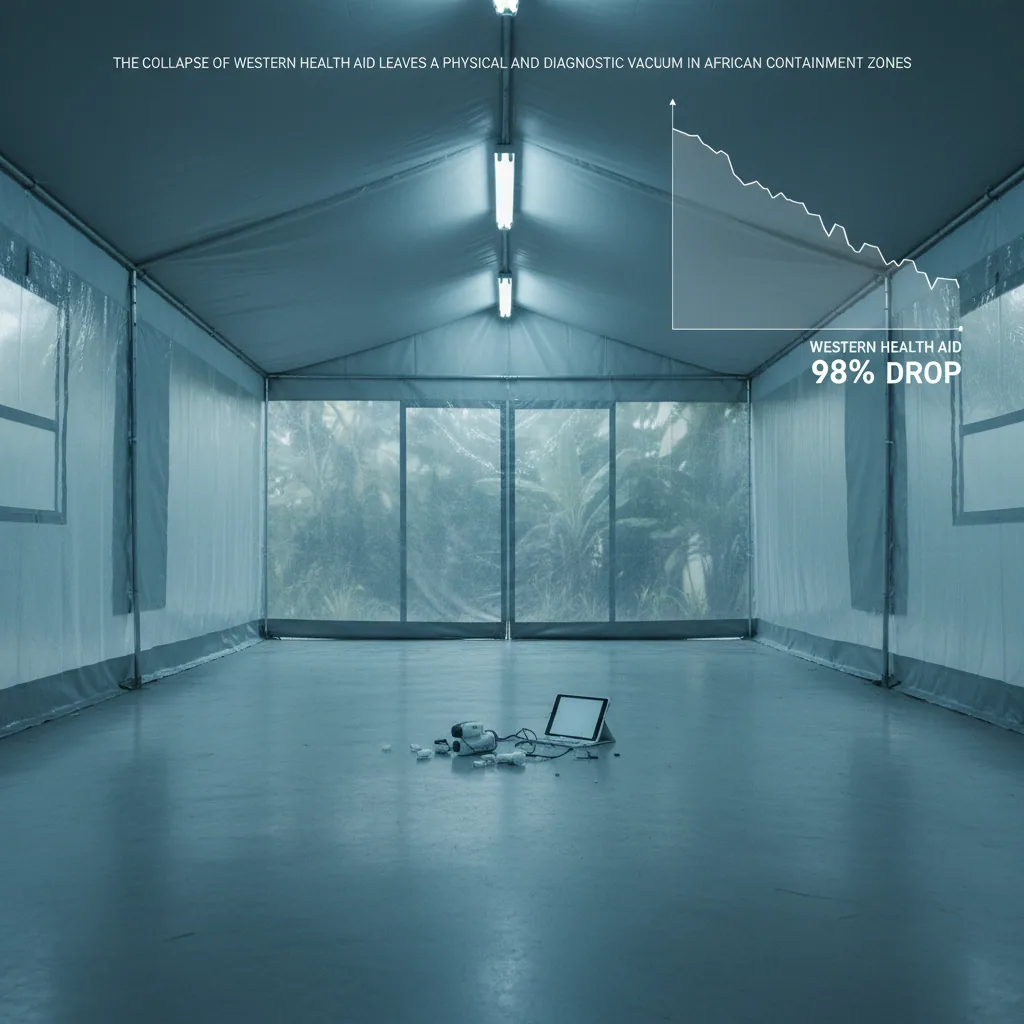
The breakdown occurs because modern biosecurity relies on delayed data and reactive border closures rather than addressing the socio-economic realities of frontline health facilities. We operate under the comforting delusion that high-resolution diagnostics provide an absolute barrier against external biological threats. This technical sophistication is rendered moot when only one in five health facilities in the Ituri Province currently has access to clean water.
On May 15, 2026, the official confirmation of a Bundibugyo virus outbreak in the Democratic Republic of the Congo shattered this perceived safety. Data indicates the virus likely circulated undetected through the Mongbwalu Health Zone for weeks prior to official confirmation. If a pathogen can traverse hyper-connected trade routes while we rely on delayed data, our socio-economic blueprint for biosecurity is fundamentally flawed.
The collapse of the traditional Fortress Strategy became undeniable when French health authorities confirmed the first European case in a doctor returning from the DRC. This cross-border correlation demonstrates that geographic isolation is a relic of the previous century. In the Estonian context, this highlights the necessity of shifting from reactive border closures to a more integrated, data-driven surveillance model.
We are witnessing the rewriting of the old order, where resource scarcity in remote regions dictates the safety of Western capitals. Can our modern legal and medical frameworks survive a world where the distance between a rural clinic and a Parisian hospital is effectively zero? This paradigm shift requires a sober re-evaluation of how we map the movement of modern biological risks.
The Bundibugyo Blind Spot: Biological Variables and the Vaccine Gap
Global health policy often treats the 2014 Zaire successes as a permanent shield, yet biological reality ignores our past victories. The Bundibugyo strain (BDBV) currently lacks a licensed vaccine or specific therapeutic treatments, rendering our existing stockpiles and containment protocols entirely irrelevant. This gap exposes the dangerous fragility of a pathogen-specific defense model that fails the moment the target shifts.
If institutional behavior remains reactive rather than structural, we will continue to sacrifice the frontline actors essential for global containment. Reports from the Africa CDC confirm at least five healthcare workers in Uganda and several in the DRC have already been infected due to early IPC failures. This failure makes the risk absolute, as high-tech medicine provides little defense if the human interface of delivery is compromised.
Current biological assessments suggest the virus has already traversed the porous borders into South Sudan, despite a lack of official confirmation from local authorities. This cross-border correlation reveals a terrifying lag between viral movement and bureaucratic data collection. In the Estonian context, this highlights how rewriting the old order of health security is a local necessity rather than a distant concern.
The emerging paradigm demands that the socio-economic blueprint of global biosecurity pivots from reactionary funding to proactive, strain-agnostic resilience. This shift requires a multidisciplinary synthesis of law and technology to mandate decentralized rapid-response capacity. How can we justify a global security strategy that relies on the dangerous hope that the next pathogen will always be one we already know how to fight?
Institutional Inertia: The Socio-Economic Blueprint of a Funding Deficit
High-stakes global declarations often collide with a vacuum of material commitment. The World Health Organization designated the outbreak a Public Health Emergency of International Concern on May 17, 2026, marking a significant legal milestone. This disconnect exposes a socio-economic blueprint where institutional behavior prioritizes symbolic rhetoric over the immediate deployment of liquid capital.
The math of failure is unforgiving as donors have committed only $90 million toward a required response budget of $518 million. In the Estonian context, if this funding gap persists, then the cross-border correlation of underfunding will prove disastrous. Such fiscal negligence would render the 2026 response a definitive failure of institutional behavior.
Beyond the ledger, the human cost of bureaucratic lag manifests in a desperate, measurable shortage of frontline medical expertise. While containment protocols necessitate a minimum of 540 trained personnel, a mere 84 individuals have been secured for deployment. This scarcity forces local healthcare workers to manage high-mortality risks without specialized support, effectively rewriting the old order through material neglect.
This paradigm shift toward persistent underfunding forces us to question the long-term viability of our current global health architecture. When the arithmetic of investment fails to meet the biological reality of a pathogen, institutional inertia creates a vacuum that border controls cannot fill. Is the international community prepared to redefine the emerging paradigm of biosecurity, or will we continue to let fiscal hesitation dictate our collective survival?
Analyzing the Ebola Protocol Failure: From Dallas to Ituri
A digital interface offers the promise of total visibility, yet high-stakes medical informatics frequently mask the very symptoms they are designed to flag. In 2014, Thomas Eric Duncan presented at a Dallas hospital with a clear travel history and acute fever. This critical data point was buried within a flawed Electronic Health Record (EHR) workflow, leading to a fatal misdiagnosis that allowed a lethal pathogen to breach an advanced healthcare system.
The subsequent infections of nurses Nina Pham and Amber Vinson exposed the sensory reality of containment breakdown. The CDC later identified that the doffing or removal of protective equipment remained the primary point of failure for these healthcare workers. The cross-border correlation of clinical errors suggests that institutional behavior has not evolved alongside our surveillance technology.
This socio-economic blueprint of failure is not merely a regional issue; it represents the emerging paradigm in how we perceive global biosecurity.
In the Mongbwalu Health Zone and across the Ituri Province, we are witnessing a repeat of these systemic vulnerabilities on a catastrophic scale. Contact tracing efforts are currently reaching only 43% to 56% of known contacts, a figure that falls dangerously short of the 90% required to break the chain of transmission. The logistical friction is palpable, with data confirming that only 19.3% of contacts in Ituri were seen within the critical 24-hour window.
Whether in the sterile hum of a Dallas trauma center or a humid clinic in Bunia, the breaking point is consistently the human-procedural interface. In the Estonian context, where we rely heavily on digital interoperability, these failures serve as a warning against technological hubris. We are rewriting the old order of pandemic response, but the data suggests we are losing the race against biological reality.
Rewriting the Old Order: Geopolitical Friction and Legal Boundaries
Global biosecurity frameworks rely on the seamless projection of medical power, yet they frequently fracture against the granite of local judicial sovereignty. In Kenya, the High Court recently issued an order to halt construction of a US-backed Ebola quarantine facility. Health Minister Aden Duale was forced to observe as a domestic legal barrier superseded an international security mandate.
This friction illustrates the emerging paradigm where traditional offshore containment models are no longer politically or legally frictionless. If global powers attempt to export biosecurity infrastructure without deep local integration, then legal bottlenecks will continue to paralyze rapid response efforts. Institutional behavior now prioritizes national legal norms over collective biological safety.
Sovereignty is the new variable. While legal battles stall physical infrastructure, the blunt instrument of regional isolation remains the desperate default for local actors. All flights to and from Bunia, the capital of the Ituri region, have been grounded to prevent the Bundibugyo strain from migrating further.
This total cessation of regional aviation creates an immediate socio-economic blueprint of decay for a territory already strained by conflict. The economic cost is absolute. This current paradigm shift reflects a world where cross-border correlation is met with increasingly rigid territorial defenses.
The Zaire-centric strategies of previous decades failed to account for this rising legal nationalism. Grounding flights may stop a virus, but it also severs the critical logistics required for medical supply chains. This rewriting of the old order suggests that biosecurity is now a matter of geopolitical negotiation rather than simple medical logistics.
The Emerging Paradigm: Data-Driven Security in the Estonian Context
Modern digital surveillance promises total visibility, yet we remain unable to track a known pathogen across a single border. While European capitals rely on sophisticated early-warning systems, current contact tracing for the Bundibugyo strain reaches only 43% to 56% of those exposed. If the WHO threshold for containment is 90%, our current institutional behavior is mathematically certain to fail the test of a globalized pandemic.
The emerging paradigm demands a multi-disciplinary synthesis of law, economics, and technology to replace the crumbling "Fortress Strategy" of national isolation. In the Estonian context, where digital infrastructure serves as our primary socio-economic blueprint, biosecurity must move beyond clinical response to incorporate data-backed future-casting. With less than 20% of the necessary funding raised, we cannot build state resilience on the promise of a vaccine that does not yet exist.
Estonian policy makers must recognize that biosecurity is now a mandatory subset of national defense and a prerequisite for economic sovereignty. In Ituri, only 19.3% of contacts were seen within the critical 24-hour window, exposing a paradigm shift where logistical failures at the source create immediate vulnerabilities in Europe. Addressing this Ebola protocol failure is the only way to prevent the cascading economic shocks of a sustained biological breach.